“All is for the best in this best of all possible worlds”
– Dr. Pangloss in Voltaire’s Candide
Whether septic shock provides a defense to the host is an open question – one that is increasingly relevant to emergency and critical care. Even if certain features of sepsis represent host defenses, It would be a mistake to think that septic shock is always adaptive for all patients and in every context.
We evolved, as did all life on this planet, and all of our ancestors survived infections long enough to give birth. However, it does not follow that we should never intervene in sepsis. We have plenty of reasons to expect non-optimal host responses to sepsis that I enumerated earlier here. The Panglossian proposal – letting nature take its course is always “all for the best” in medicine – is both a straw man argument and an example of the naturalistic fallacy. There is no room for Dr. Pangloss in the emergency department and intensive care unit.
Now that we banished Dr. Pangloss, should we also banish Dr. Osler?
- In 1913 Sir William Osler first suggested that death mostly resulted from a host response rather than the underlying pathogen
You can see Osler’s influence on the most recent sepsis consensus definition (Singer et al. JAMA 2016):

Is sepsis a dysregulated host response to infection? This is the view that motivated hundreds of pre-clinical studies and more than 100 clinical trials of immune modulating agents in sepsis. In case you have not been paying attention, let’s recall how many of these have shown a survival benefit without subsequent reversal? Zero.
The table below lists some of the failed interventions targeting the immune system in sepsis, from Marshall 2014 – Why have clinical trials in sepsis failed?

With the recent Adrenal trial, we can add one more to Marshall’s tally.
The house of medicine is full of amnesiacs. We forget “negative” trials as soon as they are published. Recalling our recent history with sepsis trials should provoke some difficult soul-searching – Was Osler wrong?
At this point the preponderance of the evidence argues against dysregulation and more for regulation.
Let’s consider sepsis bundles and early goal directed therapy. Many are unaware that the Surviving Sepsis Campaign got its start because of the marketing efforts of Eli Lilly, and was designed in part to encourage physicians to prescribe Xigris, another failed sepsis drug.
A mainstay of Surviving Sepsis until recently was the timely provision of Early Goal Directed Therapy (EGDT), a strategy of restoring blood flow and oxygen delivery to shocked organs:
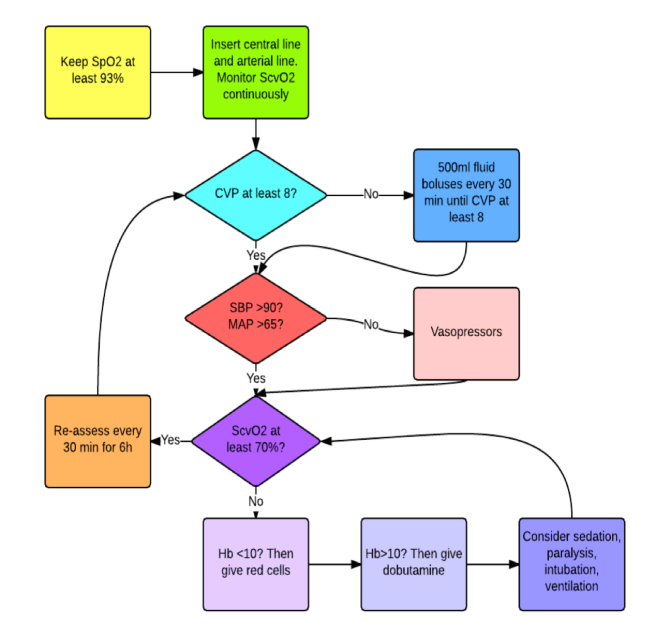
The flowchart above was derived from the famed Rivers trial, the first study to suggest a benefit to EGDT. In line with recent history of medical reversal, multiple subsequent EDGT trials failed to improve survival in recent large scale randomized trials:
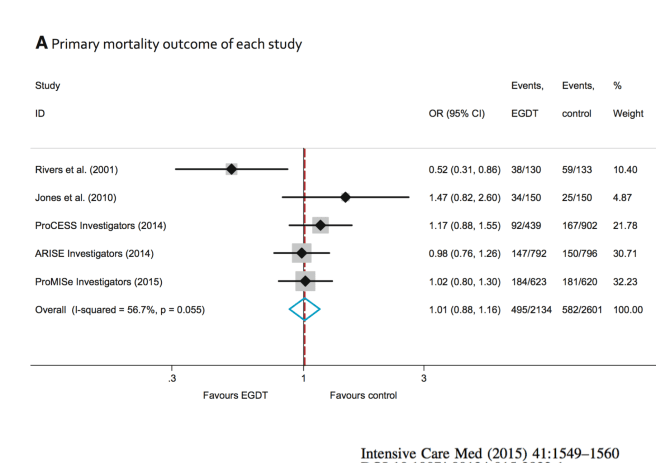
This meta-analysis result looks a lot like the ADRENAL trial:

Confronted with this powerful evidence, the Surviving Sepsis Campaign reversed course, right? Not really:
To be fair, the SSC has since de-emphasized EGDT. However, the SSC statement above betrays a business as usual ethos. Since the original Rivers trial, sepsis bundles advocated by SSC have contained useless elements – measuring SvcO2, maintaining CVP of 8 mm HG, and also demonstrably harmful ones: Xigris, dobutamine, high transfusion targets. Those elements were not included in the recent EGDT trials, as their futility had been already been demonstrated. In retrospect, early sepsis bundles were like a Trojan horse, shiny and attractive, and dangerous.
It is time to re-think sepsis.
The failure of the ProCESS, ARISE and proMISe EGDT trials to improve survival reflects the bankruptcy of the traditional conception of sepsis. EGDT was championed under the assumption of inadequate tissue oxygen and perfusion in septic shock. In fact, some recent evidence suggests that impaired tissue oxygen and perfusion may not occur in septic shock.
The recent EGDT trials also implicitly tested the hypothesis that sepsis is a dangerous departure from homeostasis. It may be that, but the demise of EGDT indicates that medical efforts to return our patients to “normal” are misguided.
We need to re-think homeostasis. Sometimes it may be good to be abnormal. Perhaps Osler was wrong after all. Perhaps we should consider that sepsis is a regulated host response, not a dysregulated one.
It is time to re-think sepsis, and rethink our treatments in light of evolution.
Next: Are we maladapted to medical treatments?
Evolution in critical care will be the topic of a special symposium during the 4th annual meeting of ISEMPH – The International Society for Evolution, Medicine and Public Health in beautiful Park City, Utah. Abstract submissions are now open.
Copyright © Joe Alcock MD
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

5 replies ›