 The ADRENAL trial is the recently published, and influential, randomized controlled trial of hydrocortisone in patients with sepsis. There are two lessons to be learned from the ADRENAL trial.
The ADRENAL trial is the recently published, and influential, randomized controlled trial of hydrocortisone in patients with sepsis. There are two lessons to be learned from the ADRENAL trial.
Lesson #1. The first is a small lesson. Should we be using steroids in sepsis? Answer: no.
This was a big study – including over 3600 patients with septic shock from 69 medical surgical ICUs in 5 countries (Australia, New Zealand, Denmark, Saudi Arabia, UK). The New England Journal article was published the same day that the study results were presented at the 2018 Critical Care Reviews conference. The bottom line:
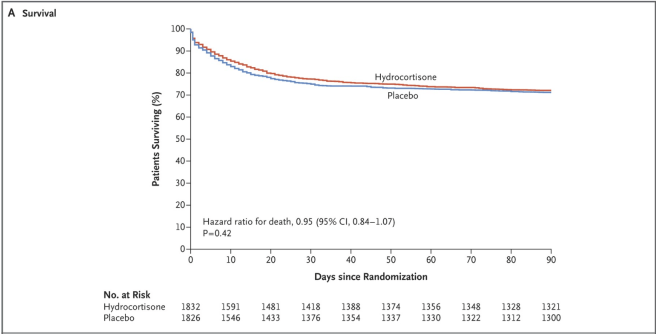
Hydrocortisone treatment did not improve survival in patients with septic shock. The intervention was also associated with a significant increase in adverse events.
This is the definitive answer. Equipoise no longer exists on the question of steroids benefiting survival in sepsis. A metaanalysis presented at the 2018 Critical Care Reviews conference confirmed the study’s main finding. No survival benefit. Subsequent trials are unlikely to be carried out.
But this is the just the small lesson of ADRENAL.
Lesson #2. The big lesson. It is time to rethink sepsis. Hydrocortisone is, after all, a treatment that targets the immune system, suppressing inflammation (in addition to other effects). The ADRENAL results call into question the idea that shock is a state of dysregulated immunity.
In the ADRENAL trial, hydrocortisone shortened the time patients were deemed to be in shock.
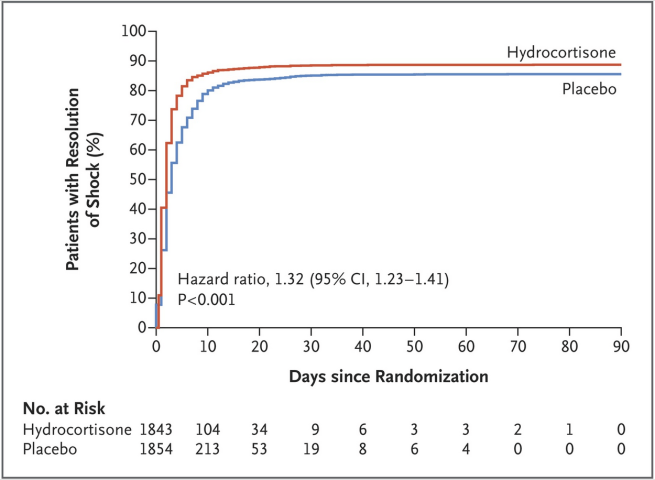
This “improvement” was illusory. The treatment made patients appear to be getting better. But they weren’t. They still died at the same rate.
One additional interesting finding was that mechanically ventilated patients receiving hydrocortisone were taken off the ventilator (extubated) faster than patients receiving placebo. This is good, right?
Not so fast. The authors write: “but taking into account episodes of recurrence of ventilation, there were no significant differences in the number of days alive and free from mechanical ventilation”
Not so good.
To recap: hydrocortisone in shock is a classic example of an intervention that makes the numbers look better, but ultimately does not help the patient.
What accounts for this failure? And why do we keep trying to find magic bullet therapies aimed at the immune system in sepsis?
The reason: sepsis researchers and clinicians have been blinded by a mistaken notion – the idea that sepsis is a dangerous overreaction of the immune system. Lewis Thomas wrote about microbes in sepsis: “It is our response to their presence that makes the disease. Our arsenals for fighting off bacteria are so powerful . . . that we are more in danger from them than the invaders.”
Does the immune system go disastrously wrong in sepsis? Getting this answer right is critically important because septic shock is a leading cause of mortality in humans. Hydrocortisone is just the most recent in a long series of sepsis trials involving anti-inflammatory agents aimed at improving survival. Only one immune modifying drug, recombinant activated protein C, ever passed through phase 3 clinical trials with FDA approval. Despite this supposed success, later definitive trials involving recombinant activated protein C showed it to be useless and it was unceremoniously yanked from the market in 2011. Another tantalizing target of inflammation in sepsis – the TLR4 pathway – resulted in spectacular failures in clinical trials, including the recent ACCESS trial. More than 10 anti-LPS/TLR4 agents were tested in sepsis. None led to successful therapies.
The ADRENAL trial is just the latest in a long series of trials of immune agents that fail to boost survival in patients with sepsis.
The history of immune agents in sepsis, taken together, suggests that natural selection favors responses to life-threats that sometimes appear excessive, but are adaptive and beneficial in the aggregate. This does not mean that every immune response in every individual is optimal. Our genomes have only an evolutionary legacy of ancestors who survived infections (at least until the age of reproduction) to guide them. For our patients, we simply don’t know how to adjust the immune response to sepsis. But it is time that we stopped acting as if we did, and spent more time trying to understand the adaptive tradeoffs that have shaped our immune systems.
The time has come to rethink sepsis in the context of evolution.
This is part 1 of 2. Coming up next. The Trojan horse of sepsis bundles.
Read also, a similar article I wrote about sepsis in the Evolution and Medicine Review.
Evolution in critical care will be the topic of a special symposium during the 4th annual meeting of ISEMPH – The International Society for Evolution, Medicine and Public Health in beautiful Park City, Utah. Abstract submissions are now open.
Copyright © Joe Alcock MD
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

Great review.
Agree with your premise that sepsis is not an “immune system doing things wrong” issue and we need to stop treating it that way (hence – nothing we do to suppress the immune system in patients trying to fight an infection has lead to an improved outcome). It is probably more of an appropriate immune response causing stress to the body that it may or may not be in good enough physical shape to handle. I have learned that the goal for treating severe sepsis and septic shock should be to lower the microbiologic burden as fast as possible while supplementing the patient’s physiologic reserve just enough so they can handle the stress of fighting the infection. Most therapies that do anything outside of those two things at best aren’t going to change mortality.
However, this does need a counterpoint because I don’t want to hear residents start saying “I thought steroids in septic shock were bad”, so here are a few observations from my perspective:
1) I get it, the steroid group didn’t have a statistically significant decrease in mortality, but they weren’t MORE likely to die either. If anything, they were 2% LESS likely to die, which would make a difference to me if I was a patient, but I won’t open the can on p-values here (fiiiine….no difference).
2) Is death really the only thing patients care about? Personally, I would like to be extubated 24 hours earlier and spend 48 less hours intubated (hours on the ventilator can be LONG and distressing), and would like to be in shock a day less (I am sure being in shock feels terrible), and I would like to be in the ICU two less days (a place no one sleeps).
3) I realize this comes with a 0.32% chance of developing either myopathy and/or encephalopathy. Would I take a 0.32% chance of either of those in order to get off the ventilator a day earlier and out of the ICU 2 days earlier? Probably. The remainder of the adverse events either 1) don’t matter to me as a patient or 2) are super unlikely to be caused by the steroid.
4) Really the only outcomes that were legitimately worse in the steroid group were having to be reintubated and maybe recurrence of shock – you don’t want those if you’re a patient. This was what they dealt with in the Meduri study for ARDS (chest 2007) – they d/c’d the steroids once the patients improved enough to be extubated and they were all back on the vent within 72 hours. In other words, steroids will improve acute physiology (especially in pulmonary disease), but they do NOT modify the disease itself. If you take them off while the disease process is still active, the patient will show you that they still have the disease by either being reintubated or going back into shock. Longer tapers may help with this problem (this study capped at 7 days).
The above said – I don’t think we should use steroids for everyone who has sepsis and is on a vasopressor like they do in this study, but if some people read the trial and they believe that decreasing the duration of mechanical ventilation and ICU length of stay is worth the relatively low risk of adverse events – I have a hard time arguing.
I have already heard some folks say “we shouldn’t use steroids in anyone with septic shock because of the ADRENAL Trial”. I couldn’t disagree more. In situations where the physiology needs to be improved to stay alive (ex. you can’t keep their BP up with vasopressors or you can’t oxygenate them on the ventilator due to ARDS) I argue that steroids should be strongly considered. It will most likely improve their acute physiology and may help them live another day. It may even get them extubated and out of the ICU faster. Again, though, because it doesn’t modify the underlying disease, don’t expect it to make them die less.
I agree with your goals of sepsis treatment – reducing the microbial burden and supporting the the patients physiologic reserve. Also you are not the first to suggest that the secondary outcome measures might be a rationale for using steroids. I can understand that thinking even if I disagree with it. But the bigger point I was trying to make is that we learn something about sepsis physiology each time a trial like this is undertaken. It is meaningful that no immune targeted drug has ever worked in sepsis. It means that our underlying assumptions about the disease are wrong.
Excellent summary and debate, thanks for having this up. My personal view is that the answer to the questions of ‘should we be using steroid in sepsis?’ does not have a binary ‘yes’ or ‘no’ answer. More a ‘well maybe in certain patients in certain situations.’ Such an ambigious position is supported by the fact that there is very much divided opinion amongst the masses. If the answer was so clear there would be unanimous concordance.
Vishal Dhokia, UK
@Dr_Dokes
Thanks for the feedback. I agree about the room for debate!