
The discovery of penicillin by Alexander Fleming ranks as perhaps the most important medical discovery of all time. Certainly antibiotics are one of the most powerful lifesaving tools in a physician’s toolkit. As we know, power can corrupt, and the indiscriminate use of antibiotics comes with a variety of downsides. We will enumerate a few of these here.
- More harm than good in self limiting infections. For many infections, the benefit of antibiotics may be limited or absent. One such example is otitis media (ear infection) in children. It remains common to prescribe antibiotics for miserable febrile children who have a bulging red eardrum on examination. Yet, research suggests we often probably shouldn’t. The terrific website NNT.com gives a good explanation of the concepts of the number needed to treat and the number needed to harm. For patients with otitis media, only 1 in 20 received any benefit (pain reduction) from antibiotics. Therefore the number needed to treat is 20 to obtain benefit. At the same time 1 in 9 will suffer significant diarrhea. The number needed to harm is 9 for antibiotic treatment in otitis media. On a population level, we are more likely to do harm than good by prescribing antibiotics to these children. Thus we should stop prescribing in most cases.
- Antibiotics cause selection for antibiotic resistance. Continuing with our otitis media (OM) example, amoxicillin is still the most recommended antibiotic. Yet, the most common pathogens causing OM- Streptococcus pneumonia, Haemophilus influenzae, Moraxella catarrhalis – show 20%, 50% and 100% resistance to amoxicillin respectively. The evolution of antibiotic resistance is an inevitable outcome of antimicrobial selection. This harm erodes the utility of our most powerful treatment options for severe infections.
- Antibiotics induce resistance in the microbiome, via direct selection and horizontal gene transfer, leaving a reservoir of dangerous resistance genes in bacteria inhabiting the microbiome. Turns out that many pneumonias and urinary tract infections have a gut origin. Evolution of resistance among these microbes may be a big problem if you develop an extra-intestinal infection from a gut microbe harboring a resistance gene.
- Antibiotics are linked with obesity. See the graphic here for a visual demonstration of this. Now I have your attention, right? Diarrhea and population level changes in resistance are old news, but obesity? Yes indeed. This effect is also likely mediated by changes in the microbiome. Korpela and colleagues recently published work showing that early macrolide antibiotic use was associated with increased risk of obesity.
- Antibiotics can cause cardiovascular death. This mortality can occur because of altered electrical conduction in the heart. e.g by the commonly prescribed medication Azithromycin. Read more here.
- Early antibiotic use may cause allergies. The increase in allergy relates to the hygiene hypothesis, which posits that decreased microbial exposure early in life alters immune development. Antibiotic exposure in early life is linked with atopy, eczema, and asthma, among others. The same Korpela et al. paper referenced above also showed a link between macrolide use and increased risk of asthma.
- Antibiotic prescriptions cause Candida infections. The reduction of antibiotic susceptible bacteria in the vagina alters pH and opens space for colonization by potential pathogens, e.g Candida. These ecological changes result in increased yeast infections in women who receive antibiotics.
- Clostridium difficile. Broad spectrum antibiotics alter the microbiome and can wipe out beneficial gut microbes that have evolved with us. This sets the stage for superinfection in the gut with the often lethal Clostridium difficile infection. C. diff, as it is commonly known, can cause life-threatening diarrhea, and results in complications that include toxic megacolon and sepsis. Infections with this organism have reached epidemic proportions in many communities. The increased incidence and increased virulence of C. diff is directly linked to antibiotic use in hospitals and in the community.
- Antibiotics use is associated with increased risk of type 2 diabetes. This phenomenon may be linked to the increased obesity from antibiotics (see above), although this association may result from other changes in the microbiome, such as decreased diversity (see below).
- Reduced microbiome diversity. Recent work has highlighted the importance of diversity within the gut microbiome for human health and longevity. Martin Blaser of NYU has made this phenomenon the focus of his career. Listen to Blaser’s description of the problem of antibiotics in this NPR segment, Modern medicine may not be doing your microbiome any favors.
In addition to these risks, antibiotics impair mitochondrial function, cause changes in blood pressure, and may result in dangerous thinning of the blood. These risks can generally be explained by evolutionary and ecological principles that we have covered in this blog. In light of these many risks, how often are these downsides explained by the doctor when you have been prescribed antibiotics in the past? Rarely, I would guess. I emphasize that antibiotics are often lifesaving and preserve good quality of life for many others. On the other hand, careful weighing of these concerns would undoubtedly result in fewer antibiotic prescriptions, with downstream benefits for individuals and the population at large.
(Disclaimer – this blog is not meant to be personal medical advice. If you have questions about your own health, you should consult your doctor!)
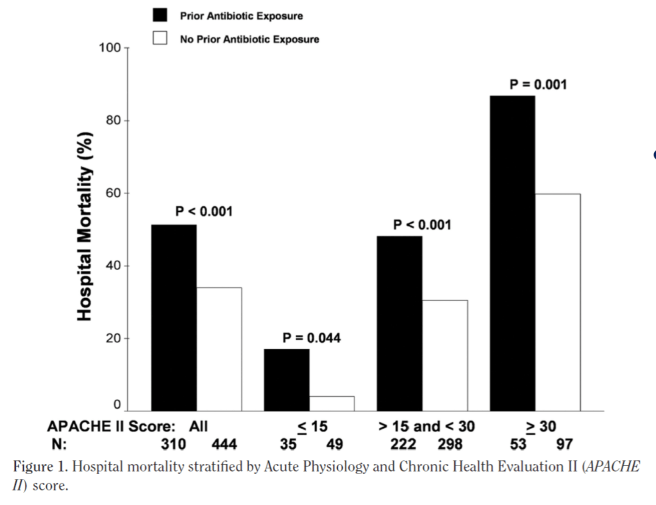
Late breaking bonus: Johnson and colleagues published an intriguing observational study in Critical Care Medicine (2011) suggesting that receiving antibiotics prior to being diagnosed with gram negative sepsis carries a significant risk of increased mortality : Impact of previous antibiotic therapy on outcome of Gram-negative severe sepsis.
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

seems like whenever a doctor claims a type of medication shouldn’t be used, they are trying to push some other form of treatment that they directly profit from.
Like what?