I recently discovered a gem of an essay by John Alverdy and Monika Krezalek published in February 2017 in the Journal of Critical Care Medicine. Entitled “Collapse of the Microbiome, Emergence of the Pathobiome, and the Immunopathology of Sepsis” it manages to touch on all of my interests, evolutionary medicine, misguided approaches to sepsis, the importance of the microbiome, and the capacity for conflict and harm from an altered microbiome, what they term the “pathobiome.” The article is unfortunately behind a paywall but I excerpt a few key bits here, with my commentary.
Alverdy and Krezalek critique the widespread idea that patients with sepsis die because of the immune system not because of the pathogen. They describe the prevailing view as:
“a pervasive immunocentric view of sepsis research – an immune/inflammatory unit/pathway must be identified that is required for mortality in any model of sepsis, because – in terms of ultimate causality – mortality is due to the response and not to the inciting pathogen.”
They go on to write that this misguided view is evident in decades of NIH funding priorities:
“Evidence for this can be easily obtained by searching the National Institutes of Health website “Grantome” using sepsis as the search word. With no exception, every funded grant is based on the immunocentric theory of sepsis and almost every grant has a promissory note that blockade of a pathway or molecule will inform a strategy to improve the outcome of human sepsis. Implicit in each of these proposals is the practice of dismissing any ongoing involvement of the inciting pathogen or any role for the ecologic collapse of the normal microbiota (microbiome) in the sepsis process. Finally, in order for the immunocentric view to prevail, the cause of death from sepsis must be believed to be due to the response itself.”
Amen! I have been arguing along similar lines for as long as I have taught evolutionary medicine at the University of New Mexico. For example, I argued that blocking pro-inflammatory pathways in sepsis is a bad idea in Disabling the smoke detector in sepsis. I wrote that we have learned the wrong lessons from sepsis research in Sepsis what have we learned, and I have an entry questioning the Underlying assumptions of sepsis treatment.
Why is the prevailing view wrong?
Because it removes any culpability from pathogens and a microbiome gone bad. The article points out that the most common animal model of sepsis (cecal ligation and puncture) kills because “normal rodent flora” spills out of necrotic intestine. Removal of the necrotic tissue and anti-microbial treatment converts 100% mortality to 100% survival. The microbiome is central to death by sepsis. As the authors point out, we never exist in a germ free state, and are either hosts to a “normal” microbiome or a virulent “pathobiome.”
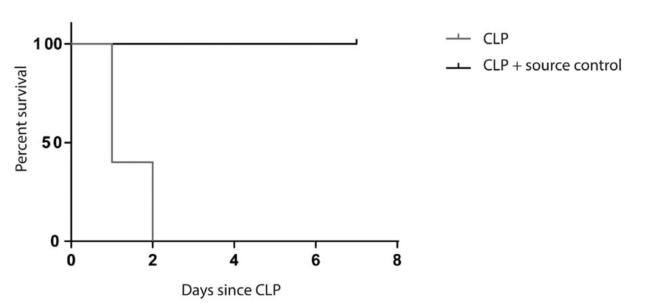
Mouse sepsis due to cecal ligation and puncture (CLP) can be reversed with proper source
control. Mortality is 100% at day 2 following CLP. Source control and supportive therapy result in 0% mortality, and all mice recover completely by day 7 (p = 0.0023; n = 5 per group) From Alverdy and Krezalek 2017.
Unfortunately, we convert healthy microbiomes to pathobiomes with abandon. This occurs when we destroy the commensal microbes using broad spectrum antibiotics, introduce hypervirulent hospital acquired pathogens, and perform procedures (intravenous lines, endotracheal tubes) that act as an on-ramp for pathogens that colonize vulnerable tissues. We physicians, surgeons, and nurses are indeed agents of selection. This selection can provoke the evolution of a harmful pathobiome.
Should we continue to ignore our role in shaping the pathobiome, and blindly pursue magic bullet therapies that block host immune defenses? No, but we undoubtedly will, believing that:
“pharmacologic interference will stop the insidious inflammatory disorder common to all sepsis. The many failures of clinical trials informed by this approach are testament to the failed thinking of this mechanistic framework. Perhaps some pathogens are simply short sighted and make the fundamental tradeoff to kill the very host upon whom their survival may depend. In some cases, this occurs rapidly, in others slowly. As one author declared “medicine needs evolution” and this is certainly the case with sepsis research.”
Here, Alverdy and Krezalek have clearly been influenced by evolutionary thinkers on health and disease, and they cite Nesse and Stearns.
It is great to read like-minded scientists on the front line of sepsis research.
Watch a video of John Alverdy lecturing on the same topic on YouTube:
Copyright © Joe Alcock MD
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

2 replies ›