About 30% of the US population gets an annual doctor exam.
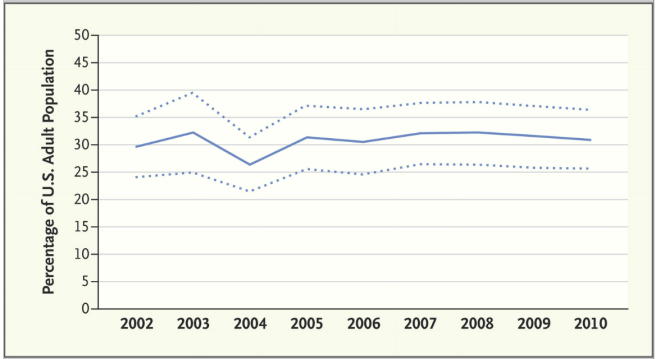
Dotted lines 95% confidence intervals. Data from, Natl. Ambulatory Medical Care Survey and Natl. Hosp. Ambulatory Medical Care Survey. Sources NEJM and Mehotra et al.
But what is the benefit of getting a check-up if you feel otherwise healthy? What does evidence-based (and evolutionary) medicine suggest you should do?
Background: You are a 39 year old male, a moderate drinker, non-smoker, who exercises at least twice a week. You indulge in fast food once or twice a week, but otherwise, you try to observe a prudent diet. Like most Americans, you have perhaps 5-10 pounds to lose. You are on no medications except occasional over the counter ibuprofen and allergy pills. You last saw a dentist 10 months ago. You last went to a doctor 9 years ago for a physical examination when you were hired.
You work in health care, and your co-workers tell you that you are crazy not to get a regular check up. Their primary doctor recommends an annual exam and they think that you should get one too. Obviously you are very overdue to get blood work and some screening tests. They tell you that you need to be responsible and go to see a doctor. Sounds reasonable right?
Lets take a moment to deconstruct that advice.
Should you get an annual physical examination? Probably not.
From the New England Journal: “Two systematic reviews summarizing both randomized trials and observational studies showed that annual physicals do not reduce morbidity or mortality, though they may be associated with reduced patient worry and increased use of preventive care.3,4
Your co-workers argue: at the very least you need to get your cholesterol and blood pressure checked!
When you were at the drug store a few months ago, you had your blood pressure checked. It was 145/85 mm Hg. Should you worry?
A recent randomized controlled trial for blood pressure reduction in intermediate risk patients (slightly elevated blood pressure, no previous heart disease) published in NEJM in April 2016 by Lonn et al. showed no benefit from starting blood pressure reducing medications (candesartan plus hydrochlorothiazide). From the study: therapy with candesartan at a dose of 16 mg per day plus hydrochlorothiazide at a dose of 12.5 mg per day was not associated with a lower rate of major cardiovascular events than placebo. The population was also older (55+) and sicker than your (hypothetical) case. Since you have no risk factors a BP lowering drug is not likely to be helpful.
And your cholesterol? your co-workers protest. You pause to think: Your older brother was just started on a statin to treat high cholesterol. Both your parents were prescribed these medications. What about you?
The excellent website theNNT.com has an excellent review of statin therapy for patients with no previous history of cardiovascular disease. Their review of systematic reviews indicates that for every 104 people given statins, 1 non-fatal heart attack might be prevented. Thus, the number need to treat to see benefit is 104. That sounds kinda good right? On the other hand, an extra case of diabetes will occur for every 100 prescriptions of statins, and 1 in 10 will suffer muscle pain. Thus the number needed to harm is 10, or 100 depending on the harm. Overall, statins are not recommended (unless you have had a previous heart attack or stroke).
Therefore, even if your blood pressure and LDL cholesterol were slightly high, you would not benefit from treatment. This leaves an open question: should you even get them checked? Probably not, at least not on an annual basis.
What should you do to stay healthy and prevent cardiovascular disease?
Eat a Mediterranean diet. In this randomized controlled trial, the hazard ratio for cardiovascular events was 0.7 for those assigned Mediterranean diets compared to control.
Put down your computer (screen time kills, my friend) and get some exercise!
Exercise vigorously – live longer
Exercise reduces the risk of 13 cancers
Late breaking update: If you are older than 75 and have high blood pressure (but not diabetes) evidence suggests that careful control of blood pressure (to a goal of 120mm Hg systolic instead of a goal of 140 mm Hg systolic blood pressure) results in fewer cardiovascular events (i.e. heart attacks) and longer life. This is a bit of a counterpoint to the evidence provided above, and reinforces the idea that all therapies should be tailored to your specific circumstances.)Read the JAMA article here:Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years
A Randomized Clinical Trial
(Disclaimer – this blog is not meant to be personal medical advice. If you have questions about your own health, you should consult your doctor!)
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

Leave a comment