Three main groups of people have lived at high elevation for generations. These are the Andeans in South America, the Tibetans, Sherpas and others living on the Himalayan plateau, and the Ethiopian highlanders living at 3000m elevation and above in north eastern Africa.
In the last few blog entries I described some of the physiologic adaptations that sea-level residents (genetic lowlanders) have in response to hypoxia. Since these operate primarily during infection and injury, but may be harmful at extreme altitude, one might predict that high altitude natives would exhibit different adaptations to altitude. This is generally true, but the story is complex.
Cynthia Beall and colleagues have described how these three different groups have different routes of adaptation to high altitude. This has been described concisely in a variety of publications, a few of which are listed here:
1. Beall An Ethiopian pattern of human adaptation to high-altitude hypoxia
“The results of this study suggest that Ethiopian high-altitude natives respond to hypobaric hypoxia differently than Andean or Tibetan highlanders.” p. 17218 Beall 2002
2. Storz Genes at High Altitude
“Andean residents at high altitude are also characterized by an elevated hemoglobin concentration. By contrast, Tibetans living at elevations of up to 4000 m present a hematological profile similar to what would be expected at sea level.” p. 40 Storz 2010.
3. National Geographic: Three high altitude people
Despite living at elevations with low oxygen content, “the Ethiopian highlanders were hardly hypoxic at all,” Beall said. “I was genuinely surprised.” p. 2 NatGeo
4. Two routes to functional adaptation: Tibetan and Andean high-altitude natives Beall-2007
“High-altitude hypoxia may be an even stronger agent of natural selection than falciparum malaria.” p. 8659. Beall 2007.
5. Beall Tibetan and Andean Patterns of Adaptation to High-Altitude Hypoxia
“Tibetan resting ventilation was roughly 50% higher than Amarya resting ventilation. For example male Tibetans had an average resting ventilation of 19.7 l/min compared to an average of 13.4 for male Amayra” p. 204 Beall 2000
To summarize:
Andeans compensate for high altitude hypoxia by making more red blood cells (mostly).

Tibetans (pictured below with Cynthia Beall) show a primarily respiratory adaptation to altitude. Their minute ventilation is greater than that of an Andean or sea level native. Their red cell numbers are not elevated and, in fact, resemble those of sea level natives.

Ethiopians do not demonstrate hypoxia at altitude remarkably, at least in comparison to Andeans and Tibetans.

Despite the lack of hypoxemia at altitude, Ethiopian highlanders do not breathe faster. Nor do they make more red blood cells.
By inference, it appears that what works for lowlander confronted by hypoxia tends to be disadvantageous for those living for generations at high altitude. I outlined how lowlanders can benefit from hypoxic pulmonary vasoconstriction, hypoxic cerebral vasodilation, hypoxic erythrocytosis, and hypoxic inflammation. These responses, triggered by common events at low altitude (infection, trauma, stroke) are linked with acute mountain sickness and chronic mountain sickness when exposed to hypobaric hypoxia of high altitude. Multiple generations of living at high altitude would be expected to require a different set of adaptations to hypoxia as compared to sea level dwellers. In fact, that is what we observe. In general, high altitude populations tend to show blunted responses to hypoxia – these may protect them from acute mountain sickness.
Some examples:
Ethiopians have blunted hypoxic pulmonary vasoconstriction and blunted hypoxic cerebral vasodilation, as shown in the figure below.

Clayden et al Circulation 2009
Oxygen stimulates less red cell production in Tibetans because of the genetic variant EPAS-1 (which codes for a different form of hypoxia inducible factor-2). This gene variant may prevent excessive erythrocytosis (aka too many red blood cells in the circulation) and play a role in reducing the risk of chronic mountain sickness. Another genetic locus EGLN1 along with EPAS1 has undergone natural selection in Tibetans thereby reducing their risk of high altitude illness.
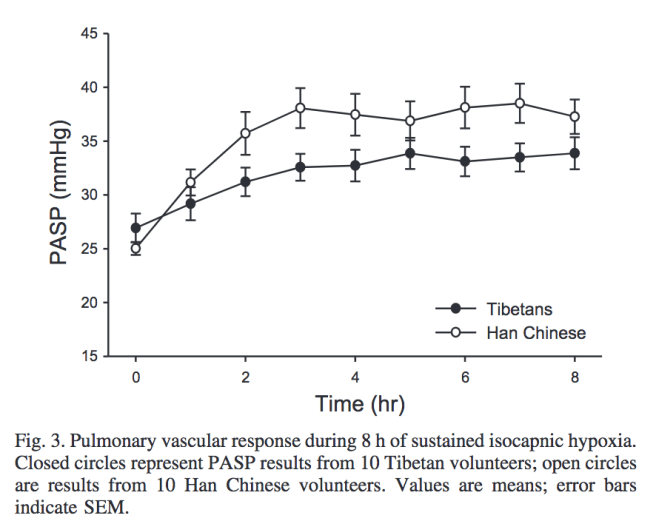
This work indicates that Tibetans have blunted pulmonary vasoconstriction to hypoxia as compared to lowland Han Chinese. Hence, lower risk for high altitude pulmonary edema.
The lesson here is that natural selection, acting on populations subjected to multiple generations of high altitude living, reduces gene-environment mismatch. Natural selection is an ongoing force that continues to shape our genes. And, in the case of high altitude dwellers, selection has made them more fit, in the Darwinian sense, to hypobaric hypoxia.
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

2 replies ›