Should we consider fever a “new normal” during infection? Should we treat it or not? A 2017 observational study of emergency department patients revealed this intriguing pattern: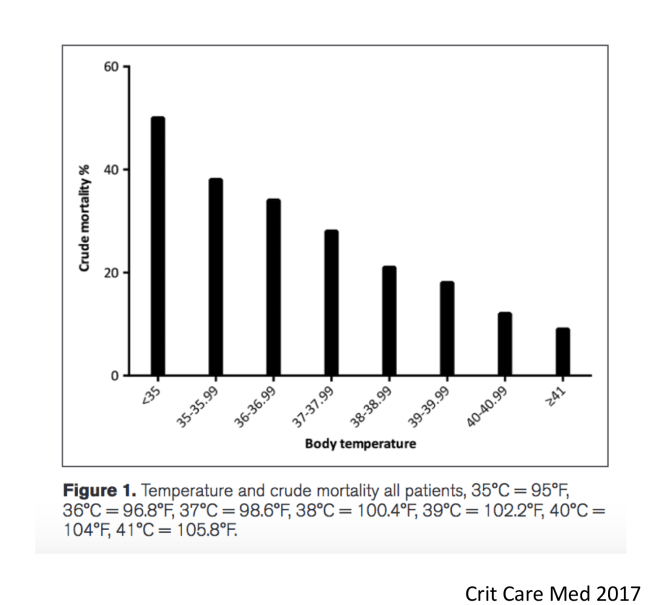 In the above study by Sunden Cullberg et al. involving 2225 patients with sepsis in Sweden, a lack of fever or low body temperature heralded a poor prognosis in sepsis.
In the above study by Sunden Cullberg et al. involving 2225 patients with sepsis in Sweden, a lack of fever or low body temperature heralded a poor prognosis in sepsis.
This will be no surprise to students of fever. In the 1970s, Bernheim, Askenase and colleagues explored the mechanism of increased survival from infection in lizards subjected to experimental fever. Lizards kept at elevated body temperature showed fewer positive blood cultures and they exhibited a greater inflammatory response that improved bacterial clearance and promoted the containment of infection.
Observational work in humans also shows a benefit to fever. Filbin and colleagues published a recent paper in the journal Critical Care showing that having a fever predicted survival in humans with septic shock.
A similar result was found in 2128 Danish patients with infection. Hospitalized acute patients with fever and severe infection have lower mortality than patients with hypo- or normothermia: a follow-up study.
Paul Young and colleagues showed that lower temperatures were associated with higher mortality among 636051 ICU patients with infection in New Zealand, Australia and the UK.
These observational trials all suffer from the limitation that association is not causation.
Actively cooling patients, however, also failed to make patients better. A recent trial involving mechanical cooling of patients with fever was recently conducted. In this recent CASS trial: “After recruitment of 436 of the planned 560 participants, the trial was terminated for futility (220 [50%] randomly allocated to hypothermia and 216 [50%] to routine thermal management). In the hypothermia group, 96 (44·2%) of 217 died within 30 days versus 77 (35·8%) of 215 in the routine thermal management group (difference 8·4% [95% CI -0·8 to 17·6]; relative risk 1·2 [1·0-1·6]; p=0·07]).”
To underline it’s result: cooling sepsis patients is not just futile, it can be deadly. (The trial was stopped early because of ethical concerns for the enrolled patients.
Acetaminophen (aka paracetamol, brand name “Tylenol”) is commonly prescribed to patients with fever. In a well designed study The Heat Trial in the NEJM, Paul Young and colleagues showed that its use in septic patients did not improve mortality. (However, acetaminophen did not apparently harm patients either.)
Taken together, perhaps at this point we have enough evidence to suggest that many patients with high temperatures are better off with their fevers than without them. Indeed, fever might be a ‘new normal’ condition that is appropriate during systemic infection.
Students of the UNM Evolutionary Medicine Elective – You have two assignments including a final writing assignment.
Write a paragraph on your response the next time you are alerted that your patient has a temperature of 101.3 F and you are asked tif you want to prescribe something for it.
For your final project: Write 1 page any evolutionary medicine topic of interest to you. For instance you could write an essay on the new normal concept – the idea that certain patient findings are more helpful and harmful, and therefore should not be “fixed.” For extra credit propose a new potential “new normal” (like fever) that might be worthy of more study.
Listen to this classic podcast by Paul Young on the topic of fever:
(Skip to minute 3:48 for the beginning of the talk)
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

1 reply ›