Proton pump inhibitors are drugs that block the hydrogen/potassium ATP-ase enzyme responsible for the secretion of stomach acid. In recent years, the prescription rate for proton pump inhibitors (PPIs) has increased from about 4% to almost 8% in the US. Many of these prescriptions are not accompanied by an appropriate indication. An additional factor driving increased use is that these medications are available over the counter in the US and in other countries, such as Denmark.
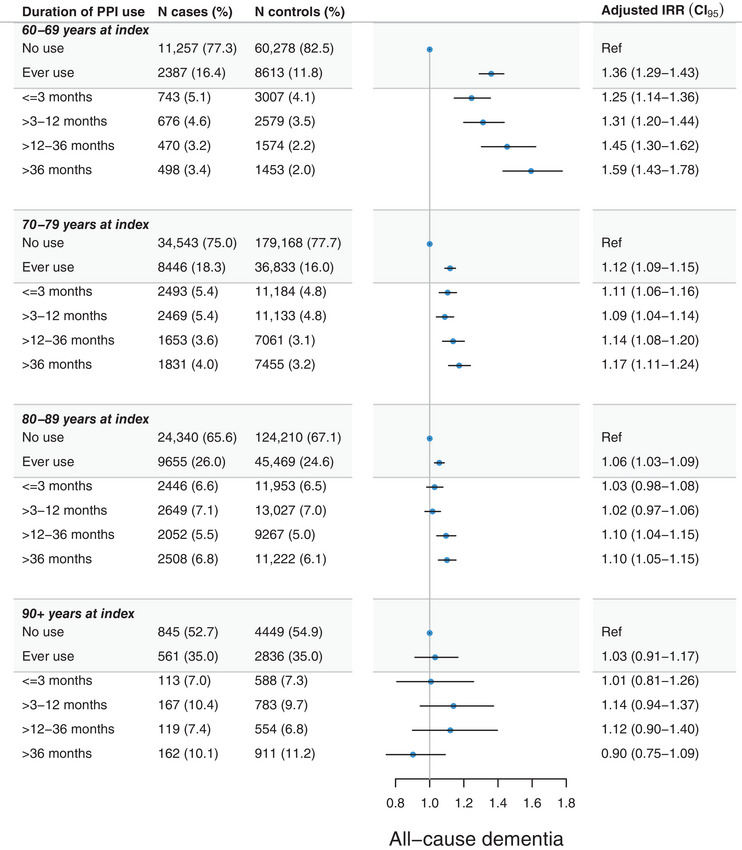
A 2024 study by Pourhadi and colleagues examined a Danish cohort of older adults numbering almost two million with a nested case-control population to see how PPI prescriptions affect dementia risk. In their analysis, PPIs were positively associated with dementia. The risk increased progressively with longer duration of prescription of PPIs and were most striking for those prescribed PPIs at younger ages – 60-69 – versus those older than 70.
Review articles citing these results have noted that the mechanism for this link is unknown, but point to the fact that PPIs cross the blood brain barrier or that they cause vitamin deficiencies potentially involved in dementia risk, like vitamin B12 deficiency.
Another possibility is that PPIs alter the community structure of the microbiota, especially in the upper GI tract. Stomach acid provides a host defense against infection and helps hosts control the population of microbes inhabiting the stomach and downstream. PPIs interfere with that defense, and users of PPIs have higher representation of oral microbes in the GI tract. At the same time, microbes in the mouth and gastrointestinal tract have been linked with a higher risk of Alzheimer’s dementia. Establishing causality between these links will require more work, but the idea that omeprazole in your medicine cabinet might increase your risk of Alzheimers down the road is bio-plausible. Other unintended consequences of PPIs exist and might happen because of harmful effects on the microbiota. I wrote about those risks of PPIs a couple years ago. Since it holds up pretty well, I decided to revisit a section of it today:
(Originally posted in June 2022) The other day I went to my local Costco. As I entered the queue of over-laden carts, emblematic of the excesses of globalized consumerism, I passed an enormous display of over-the-counter Kirkland-brand Omeprazole stacked high in eye-catching purple and pink packaging.

Omeprazole was made over the counter in 2003 but I don’t think these drugs should ever have been made available without prescription. PPIs are powerful drugs that treat heartburn by reducing gastric acid production. This is accomplished by PPI binding to the hydrogen/potassium ATPase enzyme on gastric parietal cells lining the stomach. PPIs do more than block acid. They are associated with an increased risk of congestive heart failure, kidney disease, long bone fractures, and dementia, vitamin B12 deficiency, reviewed here. Regular use of proton pump inhibitors is associated with increased incidence of type two diabetes, about 24% higher compared to non-users of the drug. Proton pump inhibitors are also linked an with increased risk of small intestinal bacterial overgrowth (which is a clue as to why these drugs can be harmful). They also increase the risk of infection by Clostridiales difficile by about 2x.
Most of these individual observational studies are unable to establish causation, but the preponderance of evidence points to PPIs causing harm. This topic is a great example of the proximate ultimate distinction. Proximate reasons involve mechanisms; ultimate reasons involve evolutionary root causes. Right now, laboratories are toiling away at the proximate molecular pathways involved in each of these associations. It is highly unlikely that they will find a shared molecular pathway linking all of these disparate harms. That might be a reason why some observers dismiss or overlook them. An evolutionary biologist, interested in why a trait evolved would take a different tack. Why did low stomach pH evolve in humans? The evolutionary biologist might test whether low pH is an adaptation of the host that tends to antagonize growth and colonization by pathogens. Studies have shown that PPIs cause pathogen overgrowth in the microbiome and increase the risk for enteric infections. This gets to the function of the hydrogen/potassium pump. The evolutionary biologist might also test whether fitness (or its proxy, survival) is reduced when we experimentally block a trait’s expression. If it is useful for humans to have a functioning hydrogen/potassium ATPase, then we would predict unintended consequences from blocking this function. In fact, substantial harms do come with PPIs, including an increased risk of death. Filling in the details with molecular pathways provides a more complete picture, but we don’t need to know exactly what the mechanisms are to make inferences about whether a trait is adaptive.
Xie et al reported an increased risk of death in long term users of PPIs – by about 1.5x. In this report, Risk of death among users of Proton Pump Inhibitors, PPI use increased mortality even more – almost 2 fold – in patients who lacked gastrointestinal conditions. (presumably that would describe most Costco shoppers who pick up an oversized package of omeprazole). Mortality differences existed even when PPIs were compared to other antacids that employ a different mechanism and are not quite as potent as PPIs.
Broadly speaking, the higher mortality risk of PPIs could result from an increase in host-microbiome conflict. If we accept Brüssow’s proposal (see the previous post for essential background) that the large intestine is the site of mutualism, and the small bowel as the site of conflict, it is easy to see how medications like PPIs could affect the host-microbiome relationship. PPIs take away the ability of the body to limit conflict in the upper gastrointestinal tract. As a result, the microbial environment is less fitness enhancing and may become fitness decreasing; ergo more deaths in PPI users. With the caveat that this does not count as medical advice, I have a very dim view of this class of medications. I do not think Costco should sell them over the counter, and I would not take them myself.
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

Leave a comment