Interferon is an innate immune molecule with an important antiviral function that provides a first line of defense against infection. Interferons are found across the tree of life, existing in all tetrapods and most fishes.
It is thought that interferon evolved first in jawed fishes, about 400 million years ago.
In COVID-19, early interest in interferon was driven by its potential role in causing harmful cytokine storms, a topic that Alix Masters and I explored in this EMPH paper titled Cytokine Storms, evolution, and COVID-19. We wrote: ‘Interferons (IFNs) induce a wide array of gene expression, including genes coding for the antiviral protein vipirin. These antiviral effector functions are important in the defense against multiple viruses. In line with the antiviral defense function of IFN, intervening to augment or stimulate the IFN response early on in infection may have therapeutic effects. A small exploratory study of 77 patients infected with SARS-CoV-2 showed treatment with IFN-α2b shortened the duration of viral shedding. Another Phase 2 trial showed that the addition of injectable IFN-β-1b, in combination therapy, was effective in suppressing the shedding of SARS-CoV-2.’
We went on to describe the contradictory approaches to interferon in COVID-19, either blocking its effects or giving the molecule itself:
‘One key example of how the immune defenses of COVID-19 can be understood as a double-edged sword is in the contradictory research on IFN as a potential target of treatment. One JAK-STAT inhibitor, tofacitinib, is currently under study for COVID-19. Tofacitinib inhibits IFN-α in vitro, providing the basis for its potential use for a cytokine storm. Targeting IFN, though, raises a red flag. Inhibition of IFN has been shown to be deleterious in other infections and may be similarly problematic in COVID-19.
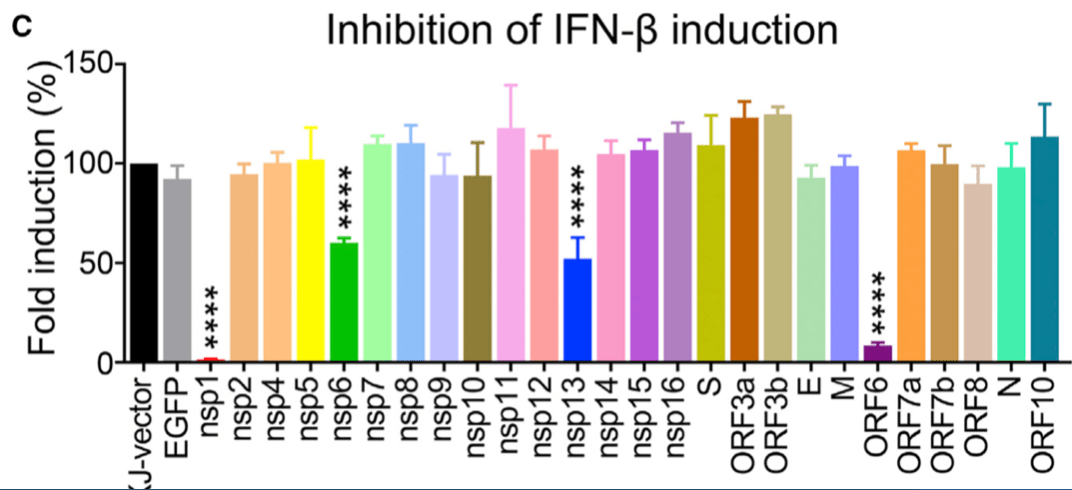
Recent work on SARS-COV-2 has revealed that inhibition of IFN is a primary virulence strategy of the virus. Like the original SARS-COV, non-structural proteins encoded by the SARS-COV-2 genome have the functional effect of reducing IFN early in infection.
Additionally, patients with genetic polymorphisms that result in impaired IFN responses have higher mortality from COVID-19. These findings suggest that it is potentially dangerous to use a treatment that disables a key antiviral defense, acting in the precise mechanism of action as the virus itself.’
Since we wrote this in 2021, the JAK-STAT inhibitor baracitinab has received emergency use authorization from the FDA. To recap, baracitinab works by blocking the pro-inflammatory effects of interferon. The well-regarded RECOVERY trial published results showing a mortality benefit in patients with severe COVID-19 infection receiving mechanical ventilation or extracorporeal membrane oxygenation (e.g. the very sickest of the sick):
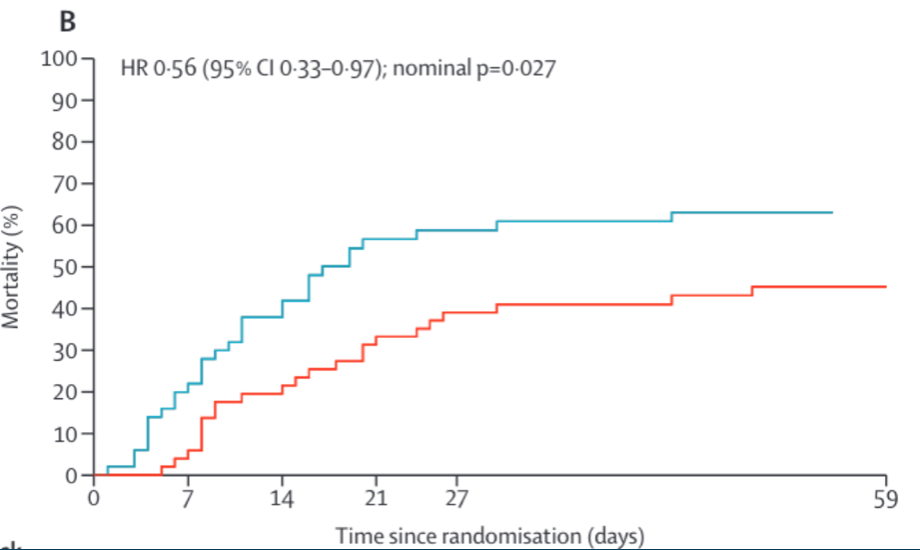
The benefit of baracitinib appears to be a solid finding, particularly in the population studied here, the very sickest COVID-19 patients in the intensive care unit on a ventilator.
As Alix Masters and I noted, JAK inhibitors like baricitinib work in the same direction as proteins encoded by the SARS COV-2 virus itself. A variety of nonstructural proteins encoded by the SARS COV-2 genome function in a way that decreases the activity of interferon in the host:
The ability of an interferon blocking drug to provide a survival benefit in COVID-19 is all the more unexpected because interferon is highest in individuals who seem to be most protected against severe disease and death – young people.

Pierce and colleagues have shown that children have far higher mucosal interferon concentrations than older adults. After swabbing children and adults, they found similar levels of virus in the nose, but children displayed far higher “expression of genes associated with IFN signaling, NLRP3 inflammasome, and other innate pathways.” Children had higher nasal IFN-α2, IFN-γ, and IL-1β protein, as compared to adults. In the nose at least, having more interferon, and higher levels of pro-inflammatory cytokines like IL-1β protects from severe disease. The adults – with lower interferon levels – had a greater need for supplemental oxygen than the children in this study and were more likely to die of the infection.
Another relevant data point is the fact that genetic variants associated with decreased interferon production are linked with mortality from COVID-19.
Severe COVID-19 seems to run in some families. Van der Made and colleagues studied 4 brothers from two unrelated families in which 2 pairs of brothers (ages 21-31) suffered severe cases of COVID-19. These researchers found that these brothers had a mutation in the gene encoding interferon, and had a markedly lower interferon response to infection. One of these unfortunate brothers with COVID-19 had a fulminant course, causing his death The others suffered complicated and severe disease involving mechanical ventilation. The likely reason for their poor outcomes: Mutations causing loss-of-function in X-chromosomal TLR7, linked with impaired type I and II IFN responses. This strongly indicates that lacking appropriate interferon responses can be deadly in COVID-19.
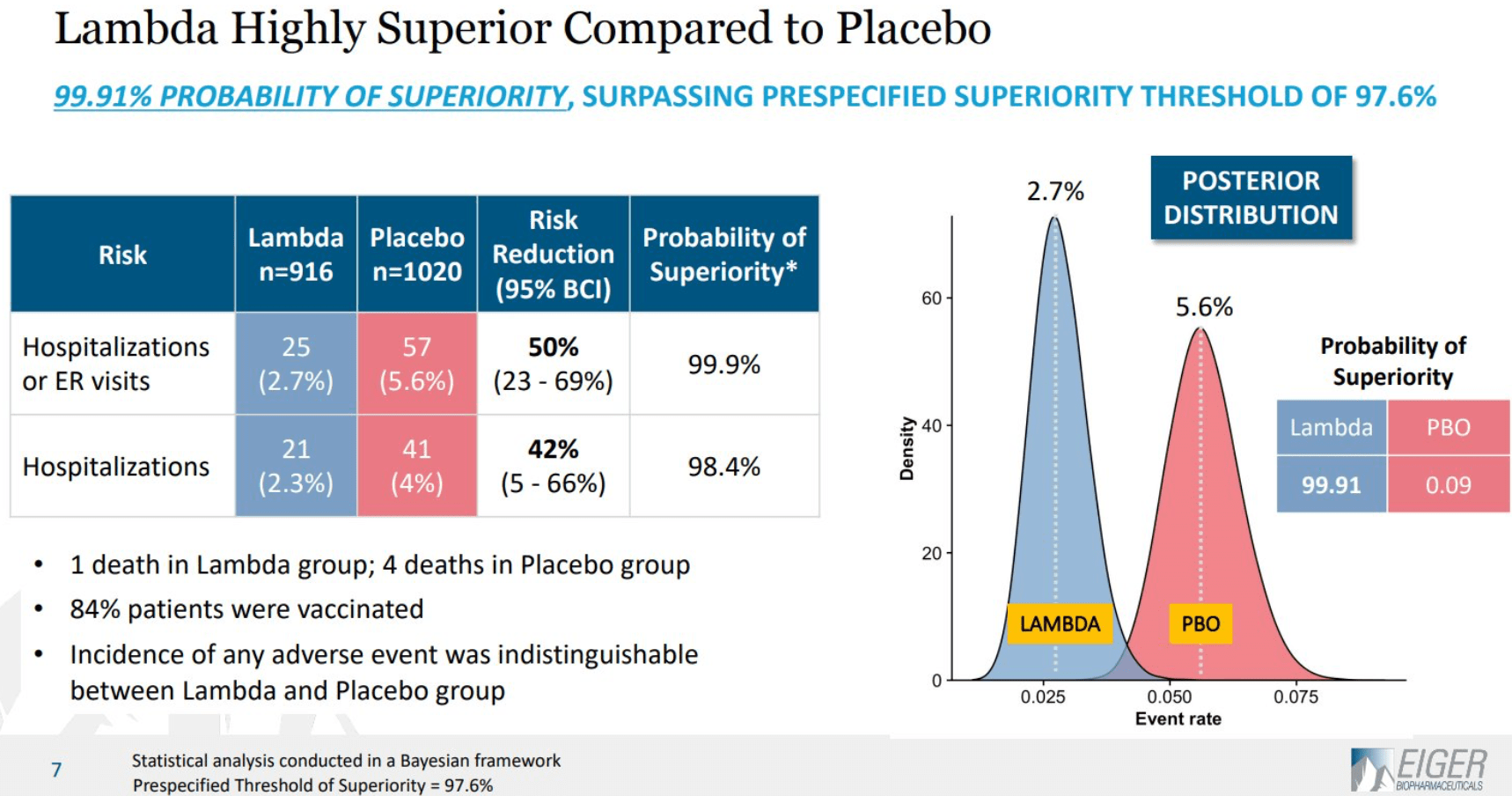
Recent results from the TOGETHER trial involving mostly vaccinated patients, showed that subcutaneous interferon treatment resulted in a 50% decrease in hospitalization from COVID-19:
These results – if they hold up – make sense in light of findings suggesting that a deficient interferon response may be to blame for severe COVID-19 pathology. In particular, the virus has been linked with the production of auto-antibodies. Raadsen et. al showed that patients who had recovered from COVID-19 had high levels of auto-antibodies against IFN-α2, the most frequently encountered interferon subtype in COVID-19 patients. These antibodies were not found in healthy controls or in ICU patients with diseases other than COVID-19. Furthermore, higher levels of interferon-α2 auto-antibodies were associated with more severe disease. Other authors have found similar results, and suggested that the existence of pre-infection auto-antibodies might predispose to severe COVID-19 infection. This is certainly possible. However, the results of Raadsen et al, are suggestive that the infection itself might cause auto-antibody formation. If so, auto-antibody production might be an adaptive virulence feature of the virus itself. Supporting this view, patients with autoantibodies also had delayed viral clearance, potentially leading to increased transmission to new hosts.
There is broad agreement that timing is important in interferon treatments for pathogenic coronaviruses. In mouse models, giving interferon early protected mice from lethal SARS-CoV or MERS-CoV; giving interferon later had the opposite results, causing hyperinflammation, reviewed here. This pattern holds up in human trials, such as the TOGETHER trial, in which interferon early led to better outcomes, while the ACTT-3 trial showed that later interferon for hospitalized adults did not improve survival. Interferon-blocking Baracitinib outcomes are the mirror image of interferon trials, with benefit only in the sickest hospitalized patients. Taken together, these results indicate that 1) first-line antiviral defenses of interferon are crucially important in protecting infected hosts from poor outcomes and 2) insufficient interferon early on can lead to worse outcomes with delayed viral clearance and harmful inflammatory damage in the lungs. Blocking inflammation with medications such as baracitinib is only helpful in late stage severe disease.
Taking an evolutionary medicine perspective (who knew!) sheds light on these otherwise contradictory observations and treatment implications. Inflammation blocking treatments only works in a small subset of patients, those whose innate inflammatory defenses are insufficient or blocked by the virus in the first place. The interactions between host and pathogen resemble a tug of war over immune modulating molecules such as interferon. The best outcomes may be achieved when these defenses are reinforced by treatments that make them more robust to viral interference, by supplying interferon early in the disease course.
Copyright © Joe Alcock MD
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

Leave a comment