In 2004, Backhed and colleagues first demonstrated that the obese, insulin resistant phenotype could be transferred from one animal to another by transferring the fecal microbiota. The investigators accomplished this by raising mice genetically predisposed to obesity under sterile conditions. Germ free mice did not become obese, despite typical energy intake and activity levels. Backhed and collegues inserted fecal pellets from conventionally raised obese mice into the food of lean germ-free mice. After this experimental inoculation, the previously germ-free mice rapidly became obese.
Others have built on those results.
Cani and colleagues (2008) demonstrated that lipopolysaccharide (LPS) – the cell wall component of gram negative bacteria – regulated the development of obesity and diabetes. Using a mouse model, Cani et al. showed that treatment with antibiotics reduced cecal LPS concentration, blocked the translocation of LPS from the gut to the blood stream, and prevented the development of pre-diabetic changes in glucose tolerance.
Vijay-Kumar and colleagues (2010) showed that mice lacking the toll like receptor 5 developed an abnormal gut microbiota that was enriched with pathogens, compared to wild-type mouse controls. These same mice developed a visceral pattern of obesity and they developed insulin resistance. The experimenters took a fecal specimen from one of these obese/insulin resistant mice and fed it to a wild type mouse. Remarkably, the inoculated mice developed a similar pattern of visceral adiposity and insulin resistance.
As we well know, results from animal studies cannot always be applied to humans. Does human data support a role of gut microbes in the development of insulin resistance and diabetes?
Humans with type 2 diabetes have important differences in the composition of microbiota, with an increase in some pathogen groups (Quin et al. 2012). A recent study of Old-order Amish in the United States showed divergence in several taxonomic groups (Zupanic 2012). Ongoing studies are underway to test whether type 2 diabetes can be cured by manipulating the composition of the microbiota.
Meanwhile, another group of researchers in France has been studying the consequences of changes in gut microbiota. Is it likely that gut microbiota could elicit selective pressure if bacteria are generally contained within the gut and don’t escape the gut and cause disease? Apart from well known gut pathogens like Salmonella, it turns out that commensal bacteria and opportunistic pathogens readily escape the intestine and find their way into the blood and tissues of mammals:
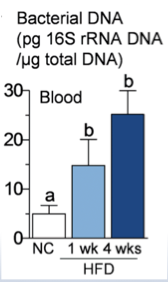
After a few weeks of a high fat diet, increasing numbers of bacteria were detected in the blood of experimental mice (Amar et al .2011). These results showed that microbiota may serve not only as a reservoir for LPS, but whole bacteria also translocate from the lumen of the gut into the bloodstream, inducing insulin resistance and diabetes.
This is an important result for two reasons. First, it shows that diet – one that causes obesity – generates the translocation of live bacteria from the gut to blood and body tissues. It might also provide an explanation for why the microbiota would trigger a systemic mobilization of resources. As others have described, insulin resistance is not an event that occurs just in the gut. Instead we find IR and inflammation in the liver, spleen, brain, skeletal muscle, and fat tissue. A body-wide immune response makes sense, only if there is a body-wide threat.
Amar’s work with mice has led to a large scale epidemiologic study of humans (2011, 2013). This work suggests that indeed, changes in gut microbiota, and blood microbiota, can predict who will develop type 2 diabetes and cardiovascular disease (Amar et al., 2013). This groundbreaking study has shown that measurable differences in blood bacteria can be found in patients who develop heart attacks. Their results include some surprises which I will describe in a later post.
These and other studies support the concept that insulin resistance co-evolved with gut microbiota, with benefits for the host in re-allocating energetic resources towards the immune system, an idea that has previously been explored by Esteve et al. (2011).
References:
Bäckhed F, Ding H, Wang T, Hooper LV, Koh GY, Nagy A, Semenkovich CF, Gordon JI. The gut microbiota as an environmental factor that regulates fat storage. Proc Natl Acad Sci U S A. 2004 Nov 2;101(44):15718-23.
Cani PD, Bibiloni R, Knauf C, Waget A, Neyrinck AM, Delzenne NM, Burcelin R. Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes. 2008 Jun;57(6):1470-81. doi: 10.2337/db07-1403.
Vijay-Kumar M, Aitken JD, Carvalho FA, Cullender TC, Mwangi S, Srinivasan S, Sitaraman SV, Knight R, Ley RE, Gewirtz AT. Metabolic syndrome and altered gut microbiota in mice lacking Toll-like receptor 5. Science. 2010 Apr 9;328(5975):228-31. doi: 10.1126/science.1179721.
Qin J, Li Y, Cai Z, Li S, Zhu J, Zhang F, Liang S, et al. A metagenome-wide association study of gut microbiota in type 2 diabetes. Nature. 2012 Oct 4;490(7418):55-60. doi: 10.1038/nature11450.
Amar J, Chabo C, Waget A, Klopp P, Vachoux C, Bermúdez-Humarán LG, et al. Intestinal mucosal adherence and translocation of commensal bacteria at the early onset of type 2 diabetes: molecular mechanisms and probiotic treatment. EMBO Mol Med. 2011 Sep;3(9):559-72. doi: 10.1002/emmm.201100159.
Amar J, Serino M, Lange C, Chabo C, Iacovoni J, Mondot S, et al.; D.E.S.I.R. Study Group. Involvement of tissue bacteria in the onset of diabetes in humans: evidence for a concept. Diabetologia. 2011 Dec;54(12):3055-61. doi: 10.1007/s00125-011-2329-8.
Amar J, Lange C, Payros G, Garret C, Chabo C, Lantieri O, Courtney M, Marre M, Charles MA, Balkau B, Burcelin R; D.E.S.I.R. Study Group. Blood microbiota dysbiosis is associated with the onset of cardiovascular events in a large general population: the d.e.s.I.R. Study. PLoS One. 2013;8(1):e54461. doi: 10.1371/journal.pone.0054461.
Esteve E, Ricart W, Fernández-Real JM. Gut microbiota interactions with obesity, insulin resistance and type 2 diabetes: did gut microbiote co-evolve with insulin resistance? Curr Opin Clin Nutr Metab Care. 2011 Sep;14(5):483-90. doi: 10.1097/MCO.0b013e328348c06d.
Categories: Uncategorized
Joe Alcock
Emergency Physician, Educator, Researcher, interested in the microbiome, evolution, and medicine

3 replies ›